
Wrist and hand diseases
Carpal tunnel syndrome
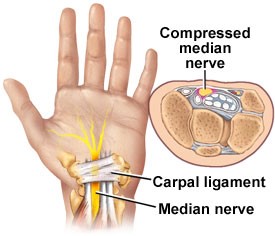
Many people who have carpal tunnel syndrome (CTS) have mild or moderate symptoms that come and go. The main symptoms of carpal tunnel syndrome are finger tingling, finger numbness or pain in parts of the hand. Pain may extend up the arm. Weak grip strength may occur and after a long period of time. Sometimes it is difficult to move your thumb or first two fingers. This is caused by excess pressure on the median nerve, which runs through the carpal tunnel in the wrist.
Carpal tunnel syndrome can be associated with any condition that causes pressure on the median nerve at the wrist. Some common conditions that can lead to CTS include obesity, repetitive wrist work, pregnancy, and rheumatoid arthritis. Sometimes these symptoms disappear again without treatment. PakSaman wrist splint can be worn for support. Sometimes symptoms are more severe when you do repetitive activities or put extreme strain on the joint – like might happen while doing work[1]. You may need to stay home from work for a while. It is important to keep moving your wrist as you normally would, but to avoid putting heavier strain on it. When worn to stabilize the wrist during sleep, a wrist splint can reduce pain and pressure on the median nerve. The least amount of pressure is placed on the median nerve when the wrist is neutral or a little extension, but unfortunately most of the activities that we do place the hand in wrist flexion or extension[2].
A splint does not always offer enough relief from symptoms, but it has virtually no side effects compared with other treatment options like corticosteroid therapy or surgery[3]. In those cases wearing a wrist splint and avoiding too much stress on the joint may be enough to provide relief[4]. Many people with carpal tunnel syndrome wear a splint at night for a few weeks to relieve mild to moderate symptoms. The splint can hold the joint in a neutral position. The symptoms are worse at night because during sleep your hand is more likely to be bent to the side. A splint can prevent this from happening. It is also important to use regular motions when moving the joint during the day to keep it from tensing up and the muscles from weakening. Sometimes it is difficult to move your thumb or first two fingers and symptom and pain bother you. This is caused by excess pressure on the median nerve, which runs through the carpal tunnel in the wrist and using thumb-wrist splint is effective.
De Quervain's disease
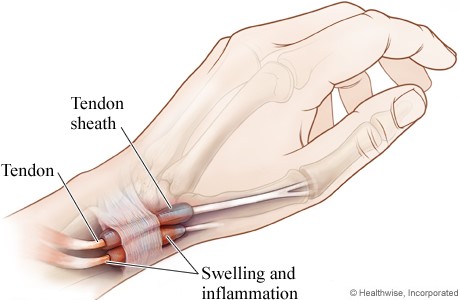
De Quervain disease is a tenosynovitis of the tendon sheath or tunnel that surrounds two tendons that control movement of the thumb. Symptoms are pain at the radial side of the wrist, spasms, tenderness, occasional burning sensation in the hand, and swelling over the thumb side of the wrist, and difficulty gripping with the affected side of the hand. The onset is often gradual. Pain is made worse by movement of the thumb and wrist, and may radiate to the thumb or the forearm[5].
De Quervain syndrome is a repetitive strain injury consider postures where the thumb is held in abduction and extension to be predisposing factors. De Quervain syndrome involves y thickening of the tendons and the synovial sheaths that the tendons run through. The two tendons concerned are those of the extensor pollicis brevis and abductor pollicis longus muscles[6]. Palliative treatments include a thumb-wrist splint that immobilized the wrist and the thumb to the interphalangeal joint and anti-inflammatory medication[7]. Also if symptom observe just in thumb, Thumb Spica Splint is a convenient orthosis designed to keep the thumb in the functional i.e. abduction position. It supports the CMC joint and immobilize the MCP joint of the thumb without inhibiting hand movement. Helps reduce pain and inflammation and prevents further thumb injury.
Triangular Fibrocartilage Tear
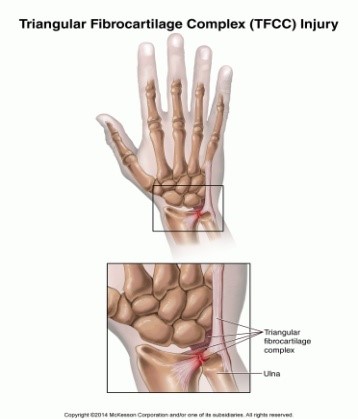
The triangular fibrocartilage complex (TFCC) is located between the ulna and carpals. With the disc, the radius bears 60% of loading; without the disc, the radius transmits 95% of the loading. This cartilage may be progressively damaged when compression and rotation forces are continually being placed on the wrist. These forces are commonly experienced in the wrists of gymnasts and racquet sport players. Symptoms include swelling and pain on the little finger side of the wrist. Wrist Brace or wrist splint, rest and anti-inflammatory treatment may be required.
Basal thumb arthritis
The carpometacarpal (CMC) or trapeziometacarpal joint of the thumb allows a wide range of movement in three planes. This increase in mobility, however, renders the joint prone to degeneration. Basal thumb arthritis is a common problem that presents to hand clinics. Typically, patients have pain localized to the base of the thumb, often radiating to the thenar eminence and the metacarpophalangeal (MCP) join. Most patients, regardless of the severity of the disease, will benefit from an initial period of conservative management. The hand is rested by immobilizing the base of the thumb in a thumb spica splint.

Wrist sprain
Wrist joint is composed of eight small carpal bones and the bones of the forearm, which together make up the wrist joint. This joint needs both strength and mobility because of the diversity of tasks and activities. However, there are numerous complications related to this area. The purpose of a wrist support is to provide support to the wrist joint during heavy or repetitive movements and helps to athletic wrist during exercising. During these movements, the wrist can be pulled into excessive extension under load and result in possible injury. Wrist support compresses the area and retains the heat to allay local pain and inflammation. Depending on your activity, you can use adjustable elastic wrist support or PakSaman neoprene wrist support.
1. Carlson, H., et al., Current options for nonsurgical management of carpal tunnel syndrome. International journal of clinical rheumatology. 5(1): p. 129-142.
2. Burke, D.T., et al., Splinting for carpal tunnel syndrome: in search of the optimal angle. Archives of physical medicine and rehabilitation, 1994. 75(11): p. 1241-1244.
3.Huisstede, B.M., et al., Carpal tunnel syndrome. Part I: effectiveness of nonsurgical treatments–a systematic review. Archives of physical medicine and rehabilitation. 91(7): p. 981-1004.
4. Page, M.J., et al., Splinting for carpal tunnel syndrome. The Cochrane Library.
5. Ilyas, A.M., et al., De quervain tenosynovitis of the wrist. Journal of the American Academy of Orthopaedic Surgeons, 2007. 15(12): p. 757-764.
6.Stahl, S.p., et al., Systematic review and meta-analysis on the work-related cause of de Quervain tenosynovitis: a critical appraisal of its recognition as an occupational disease. Plastic and reconstructive surgery. 132(6): p. 1479-1491.
7.Coldham, F., The use of splinting in the non-surgical treatment of de Quervain's disease: a review of the literature. The British Journal of Hand Therapy, 2006. 11(2): p. 48-55.
Your comment successfully stored, thanks. Unfortunately comment storage process failed.